
Heart Health After Menopause: Why Cholesterol Is Only Part of the Story
If you've arrived at this article because your cholesterol went up and you weren't sure why, there's a good chance the answer is hormonal. Perimenopause-related cholesterol changes are real, well-documented, and largely under-discussed in clinical settings. Understanding them as part of a broader biological picture, rather than a dietary or lifestyle failure, is the first step toward a genuinely informed response.
Heart disease isn't explained by cholesterol alone. High LDL significantly raises risk and the evidence for that is strong and consistent. But whether that risk actually leads to disease depends on the health of your artery walls, the degree of inflammation in your body, your hormonal environment, your sleep and daily rhythms, and a complex web of factors that a single number on a blood test simply can't capture.
Statins are powerful, evidence-based medicines that genuinely save lives. Understanding how they work, what side effects to watch for, and what the CoQ10 connection means in the context of perimenopause allows for a better, more informed conversation with your healthcare provider.
And the natural strategies outlined here aren't alternatives to good medicine; they're complements to it. This is integrative heart care, rooted in evidence, attentive to the whole person, and especially relevant to the distinct biology of women in midlife.
NOTE: This article is not intended as medical advice. See your primary practitioner for advice about your health as this article is general in nature and does not consider individual circumstances.

Heart Health After Menopause: Why Cholesterol Is Only Part of the Story
Evidence-based · 25 peer-reviewed references · 15 min readIf you’ve recently had a routine blood test and been told your cholesterol has gone up, and you’re somewhere in your 40s or early 50s - there’s something important your doctor may not have mentioned: that rise in LDL cholesterol (often referred to as ‘bad’ cholesterol) may be one of the first biological signals that perimenopause has begun.
This isn’t a reason to panic. It’s a reason to understand what’s happening in your body, and why the standard story about cholesterol and heart disease is far more nuanced, and more interesting - than a single number on a lab report.
Heart disease is the leading cause of death in women over 50. But the biology behind it involves far more than cholesterol. This guide walks through the oestrogen-cholesterol connection, how your artery walls work, the role of inflammation, what statins actually do, and the evidence-based natural strategies that support a healthy heart through midlife and beyond.
QUICK ANSWER
Cholesterol commonly rises during perimenopause because oestrogen levels are falling, and research suggests it may be one of the earliest signs of this hormonal shift. Heart disease risk in women is also shaped by damage to the inner lining of blood vessels, inflammation, and disrupted sleep patterns. This guide covers all of it, including practical natural strategies
What’s in this article
• Why cholesterol rises in perimenopause and what the research says
• What genetic research on cholesterol actually tells us
• Your arteries' living inner lining, and why it matters
• The glycocalyx: a tiny protective coating with a big job
• Inflammation and how plaque really forms
• Statins: origins, how they work, and what to watch for
• Evidence-based natural strategies for heart health
• Sunlight, body clocks, and the heart
• FAQ: your questions answered
• Glossary of key terms
1. Why cholesterol rises in perimenopause, and what the research says
Firstly, let’s not forget - WE NEED CHOLESTEROL! It is what our sex hormones, and steroid hormones (cortisol, adrenaline etc.) are made from.
For many women, the first sign that perimenopause has begun is not a hot flush. It's not a missed period. According to a growing body of research, it may be an unexpected rise in LDL cholesterol showing up on a routine blood test, often before any other symptoms are noticed.
This isn't widely known in general practice, and many women are prescribed cholesterol-lowering medication or sent away with dietary advice without ever being told that their cholesterol change may simply be their hormones shifting.
KEY POINT:
Several large, long-running studies now confirm that rising LDL cholesterol is one of the most consistent early signs of the menopause transition, and that it is driven by hormonal change, not simply by getting older or eating differently.
The oestrogen–cholesterol connection
Oestrogen plays a direct and protective role in how the body manages cholesterol. It helps the liver clear LDL out of the bloodstream more efficiently, supports the production of HDL ('good' cholesterol), and has a calming, anti-inflammatory effect on blood vessel walls. When oestrogen levels begin to fluctuate and fall during perimenopause, all of this protection begins to fade.
The result is a predictable shift: LDL and total cholesterol rise, triglycerides (blood fats) go up, and HDL, although it may temporarily increase, gradually starts to lose its protective properties over time.
What the landmark research found
The most comprehensive evidence comes from the Study of Women's Health Across the Nation (SWAN), the largest American study to follow women continuously through the menopause transition. SWAN tracked 2,659 women over nearly four years, looking at cholesterol levels alongside hormonal changes (Wildman et al., 2004; Matthews et al., 2017).
Its findings were striking: cholesterol rose most sharply right around the time of a woman's final period. And crucially, this wasn't simply an age thing; it was tied specifically to the hormonal shift, not to the passage of time itself.
A study following Korean women through the same transition found that total cholesterol and LDL rose by around 11% and 19% respectively during perimenopause, with the rise in FSH (a hormone that climbs as the ovaries begin to wind down) being one of the triggers (Hirose et al., 2011). FSH is often one of the very first measurable signs of perimenopause, and it appears to set off the cholesterol changes that follow.
The Pittsburgh Healthy Women Study, which followed 372 women and published its findings in Stroke (Matthews et al., 2001), found something particularly sobering: the cholesterol rises during perimenopause were greater than at any other life stage, and the cholesterol levels women had before menopause could predict how much artery narrowing they would have five to eight years later. The perimenopausal window appears to be a key period of vulnerability for the heart.
Why this matters in practice
For a woman in her 40s whose cholesterol has suddenly risen without obvious reason, these findings raise an important question worth discussing with a healthcare provider: could this be perimenopause? Hormone levels can swing wildly from day to day in early perimenopause, making a single hormone test unreliable. Cholesterol trends, by contrast, are more stable and may actually give a clearer picture of where a woman is hormonally.
A rise in LDL in a perimenopausal woman is not automatically a lifestyle failure or a signal to immediately start medication. It may instead be a prompt to look at her overall heart health more broadly, including signs of inflammation, blood vessel health, blood pressure trends, coronary artery calcium score, and the full hormonal picture.

BOTTOM LINE
If you're in your 40s and your cholesterol has recently risen, particularly if you've also noticed changes in your cycle, sleep, or mood, it's worth raising the possibility of perimenopause with your doctor. A rising LDL may be your body's first visible signal of hormonal change, not simply a diet problem.
2. What genetic research on cholesterol actually tells us
Large-scale genetic studies make a convincing case: high LDL cholesterol significantly raises the risk of heart disease. Studies that use inherited genetic variations as a kind of natural experiment have shown that people born with genes that cause lifelong high LDL have substantially higher rates of heart disease (Ference et al., 2017).
But here's what's interesting: even within these high-risk groups, not everyone develops heart disease early in life. And people with familial hypercholesterolaemia (FH), a genetic condition that causes very high LDL from birth, often don't develop narrowed arteries until midlife or later. The condition of the artery wall itself turns out to matter just as much as the cholesterol level.
Familial hypercholesterolaemia (FH) and the age-65 milestone
One of the more surprising findings in FH (family related high cholesterol) research is particularly relevant to women approaching or going through menopause: making it to a certain age without a heart attack or stroke may itself be a meaningful sign of resilience. Scientists studying a large group of French-Canadian women with FH identified age 65 as a key milestone. Women who reach it without a cardiovascular event appear to be a distinct 'survivor' group, likely protected by biological factors that have kept their arteries in better shape despite high cholesterol throughout their lives (Khoury et al., 2021).
A Norwegian study tracking nearly 5,000 people with genetically confirmed FH found that while death from heart disease was significantly higher than average in younger age groups, this excess risk had largely disappeared by the time people reached their seventies and was actually lower than in the general population (Mundal et al., 2014). A larger follow-up study of over 5,500 FH patients confirmed the pattern: the elevated risk that dominates early adulthood keeps falling with each decade, eventually reversing in older age (Mundal et al., 2017). For women with FH who get through the higher-risk years around menopause with their heart health intact, the picture appears to improve considerably.
KEY POINT
High LDL is a major risk factor, but whether it actually leads to narrowed arteries depends significantly on the health of the artery wall itself. Two structures are particularly important: the endothelium and the glycocalyx.
3. Your arteries' living inner lining
Think of the inside of your blood vessels as having a living skin, just one cell thick, called the endothelium. It's not just a passive lining; it's a remarkably active layer that controls how blood vessels relax and tighten, manages clotting, and regulates inflammation. A healthy endothelium continuously produces a gas called nitric oxide, which:
• Relaxes and widens blood vessels, allowing blood to flow freely
• Prevents blood cells from clumping together inappropriately
• Damps down inflammatory signals in the vessel wall
• Stops immune cells from sticking where they shouldn't
When nitric oxide production falls, because of oxidative stress, high blood sugar, smoking, ageing, or high blood pressure, the vessel wall starts to malfunction. It becomes stickier, more leaky, and more reactive to inflammation. This is the very first stage in the development of fatty plaques in the arteries (Gimbrone & Garcia-Cardena, 2016).
Oestrogen directly supports nitric oxide production and helps blood vessels stay relaxed and flexible. When oestrogen falls during perimenopause, this protection is withdrawn, adding another layer of vulnerability on top of the cholesterol changes already under way.
WHY IT MATTERS
The ability of your blood vessel lining to produce nitric oxide is a direct reflection of vascular health, and it can be improved through diet, exercise, and certain natural compounds.
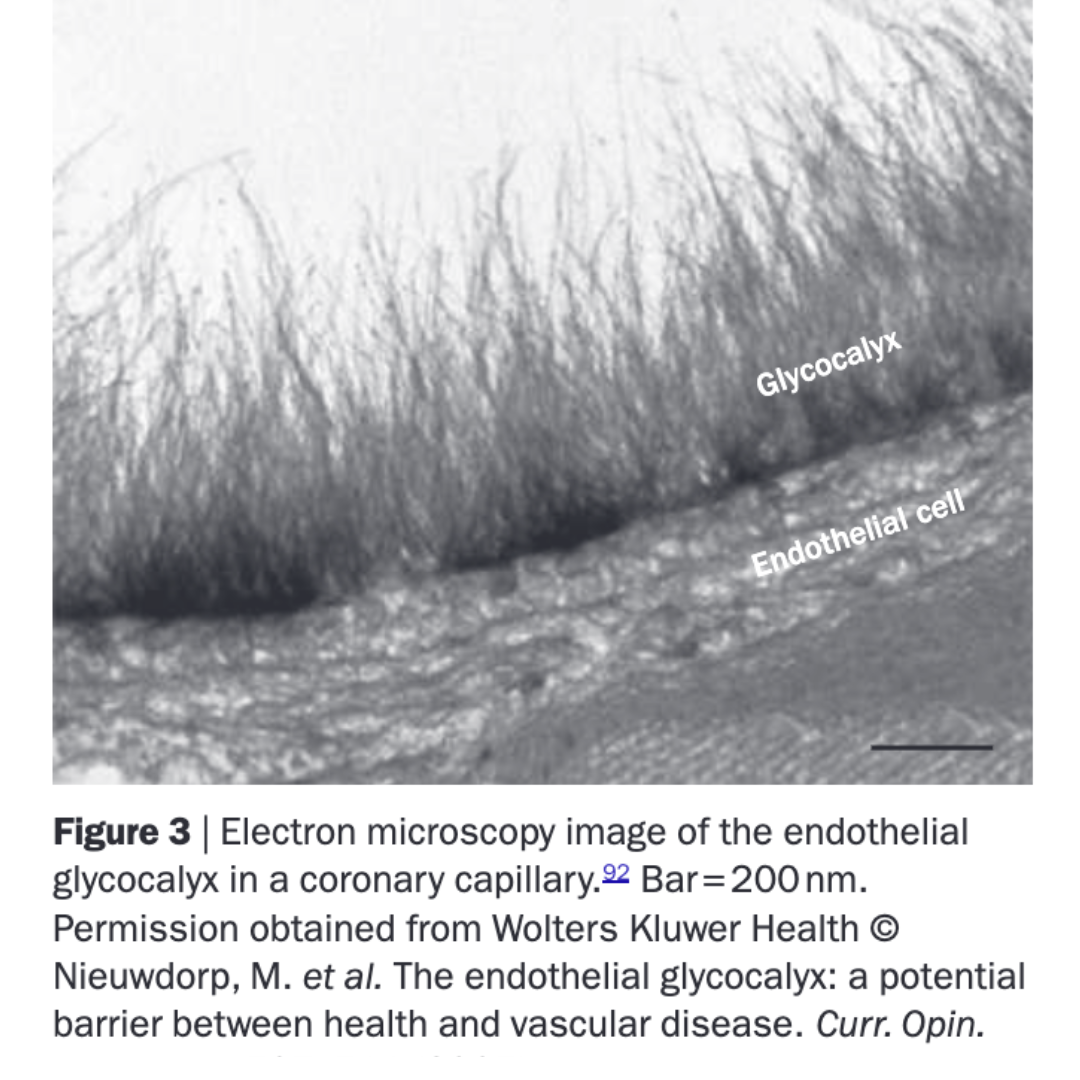
The glycocalyx, a microscopic layer lining the inside of all blood vessels, and vital to protecting that lining.
The glycocalyx: a tiny protective coating with a big job
Sitting right on top of the endothelial cells is an ultra-thin, sugar-based coating called the glycocalyx. You can't see it with the naked eye, but it plays a critical role in keeping the artery wall healthy:
• It acts as a protective barrier, preventing LDL cholesterol from making direct contact with the vessel wall
• It detects changes in blood flow and uses that information to trigger the release of nitric oxide
• It prevents immune cells and blood platelets from sticking inappropriately to the vessel wall
• It regulates how permeable (leaky) the vessel wall is
The glycocalyx can be damaged by diabetes, high blood pressure, ongoing inflammation, and high blood fats (Yilmaz et al., 2019). Once it's worn down, LDL cholesterol can get much closer to the vessel wall, speeding up the process by which plaques begin to form.
This also explains why plaques tend to develop at the bends and branches of arteries, where blood flow is more turbulent and the physical stress on this delicate coating is greatest.
5. Inflammation and how plaque really forms
Decades of research have shown that the build-up of plaques in the arteries is as much about inflammation as it is about cholesterol. The process isn't simply 'cholesterol sticks to the artery wall.' What actually happens is more like this: LDL that has been chemically damaged (oxidised) enters a vulnerable vessel wall, sets off an immune response, and triggers a slow-burning inflammatory process that gradually builds into a plaque (Libby, 2002).
It is tempting to think of cholesterol as the villain in this story, but the science tells a more nuanced tale. Leading cardiovascular researcher Professor Peter Libby of Harvard Medical School has shown that our understanding of how arteries become damaged has been completely transformed in recent years: rather than a simple problem of too much cholesterol, the formation of artery-clogging plaques is now understood to be deeply driven by inflammation and injury within the artery wall itself (Libby, 2021a, 2021b). In other words, cholesterol may be arriving at the scene as part of the body's attempt to repair existing damage, much like blaming the firefighters for a fire simply because they are always found at one. This idea has solid scientific roots (Ross, 1999), and was powerfully confirmed when a large clinical trial involving over 10,000 patients showed that targeting inflammation alone, without touching cholesterol levels at all, still significantly reduced the rate of heart attacks and strokes (Ridker et al., 2017). For women in midlife, where inflammation tends to rise alongside shifting hormones, this broader picture of what actually drives cardiovascular risk is well worth knowing about.
BOTTOM LINE
Rather than a simple blocked pipe, artery disease is better understood as a slow inflammatory process happening in a vulnerable vessel wall, one that cholesterol alone does not fully explain.

KEY INSIGHT
Nitric oxide released from the skin in response to sunlight directly supports blood vessel health and the integrity of the glycocalyx, both of which are under extra pressure during the menopause transition.
6. Statins: origins, how they work, and what to watch for
A surprisingly fungal origin
Statins are among the most widely prescribed drugs in the world, but their origins might surprise you. The first statin was discovered in 1976 by Japanese biochemist Akira Endo, who isolated it from the fermentation broth of a blue-green mould called Penicillium citrinum. His thinking was clever: if moulds compete with cholesterol-producing organisms in nature, they may have evolved natural chemicals to block their rivals' cholesterol production (Manzoni & Rollini, 2002).
How statins work
Statins work by blocking a key enzyme in the liver that the body uses to make cholesterol. When this enzyme is blocked, the liver responds by pulling more LDL out of the bloodstream to compensate, which lowers circulating LDL levels. Beyond that, statins also have broader effects: they reduce inflammation, help blood vessels function better, and may help stabilise existing plaques, which could partly explain why they work as well as they do beyond simply lowering cholesterol.
Side effects worth knowing about
NOTE: Speak to your doctor before changing any medications - this article is for information purposes only.
Statins are well-studied and genuinely reduce the risk of heart attacks and strokes. But like any medication, they come with side effects worth understanding:
• Muscle symptoms: The most commonly reported side effect is muscle pain, weakness, or cramping. Research suggests that CoQ10 supplementation may help with this, because statins reduce the body's natural CoQ10 levels as a side effect of the same mechanism that lowers cholesterol (Kovacic et al., 2025).
• CoQ10 reduction: CoQ10 is a substance the body makes naturally and needs for energy production inside cells. Statins reduce it as an unintended consequence. This is particularly worth knowing during perimenopause, when the body's energy systems are already under hormonal pressure.
• Diabetes risk: Multiple large analyses have found a modest but consistent increase in new-onset type 2 diabetes in people taking statins, especially at higher doses (Casula et al., 2017). Women appear to be at slightly higher relative risk than men.
• Eye pressure: Emerging research has found links between long-term high-dose statin use and raised pressure in the eye, which is a risk factor for glaucoma (Pan et al., 2025). This remains an active area of investigation.The Ethical & Emotional Angle
7. Evidence-based natural strategies for heart health
Good integrative care isn't about rejecting conventional medicine; it's about building the fullest possible toolkit. Several dietary, herbal, and lifestyle strategies have solid clinical evidence behind them, and are particularly relevant for women navigating the hormonal changes of perimenopause and beyond.
Hibiscus tea
Clinical trials show that drinking hibiscus tea regularly can significantly lower both the upper and lower numbers in a blood pressure reading in people with mildly to moderately raised blood pressure, with effects comparable to some blood pressure medications (McKay et al., 2010). It appears to work by relaxing blood vessels and acting as a mild diuretic.
Bergamot extract
Studies using a concentrated extract from bergamot (the citrus fruit that gives Earl Grey tea its flavour*) have shown reductions in total cholesterol, LDL, and blood fats, alongside increases in HDL. It appears to work through a similar mechanism to statins, while also acting as an antioxidant (Mollace et al., 2011), making it a particularly interesting option for women dealing with perimenopausal cholesterol changes. Practitioner only supplements can be prescribed by your naturopath or GP.
*sadly, most Earl Grey tea often has ‘natural flavours’ which is another way of saying it’s artificial flavouring, and therefore won’t help reduce cholesterol.Red yeast rice
Red yeast rice naturally contains compounds that work in the same way as statin drugs to lower cholesterol production in the liver. A randomised clinical trial in China found significant reductions in heart disease events with red yeast rice supplementation (Lu et al., 2008). Because it works similarly to statins, the same cautions apply, and it's best used under professional guidance.
Mushrooms and beta-glucans
Oyster mushrooms and certain other medicinal mushrooms contain soluble fibres called beta-glucans, which have been shown in research to lower total and LDL cholesterol by reducing the amount of fat absorbed from the digestive system (Khatun et al., 2007).
Dietary fibre
Soluble fibre from oats, beans, psyllium husks, and flaxseed consistently lowers cholesterol in well-controlled studies (Anderson et al., 2000). It also supports the gut microbiome, which plays a growing and important role in how the body processes and recycles oestrogen. This connection between gut health, oestrogen, and cholesterol is particularly relevant for perimenopausal women.
Nitrate-rich vegetables
Leafy greens and beetroot are rich in natural nitrates* (not to be confused with nitrites found in processed meats), which the body converts into nitric oxide, helping blood vessels stay relaxed and blood pressure in check (Kapil et al., 2015).
Lifestyle factors that protect the artery wall
• Regular aerobic exercise stimulates blood flow through the vessels, which directly triggers nitric oxide release and helps maintain the health of the protective glycocalyx coating
• Keeping blood sugar stable reduces the chemical damage (oxidative stress) that wears down the glycocalyx; even modest improvements in blood sugar control are beneficial for the heart
• Good quality sleep and keeping a regular daily rhythm directly influence inflammation and metabolic health
• Omega-3 fats (from oily fish, flaxseed, or walnuts) and plant foods rich in polyphenols (berries, olive oil, dark chocolate) reduce the underlying inflammation and oxidative stress that damages blood vessel walls
8. Sunlight, body clocks, and the heart
It's been known for decades that heart disease is more common in countries further from the equator, and that rates rise in winter. Two biological mechanisms, one involving sunlight and the skin, the other involving the body's internal clock, are increasingly understood to explain why.
Sunlight and blood pressure: a skin-based mechanism
Sunlight reduces blood pressure.
This is a widely acknowledged fact, taught in medical colleges globally, however until recently the method of action was unknown. Research from the Universities of Edinburgh and Southampton showed that when UVA rays from sunlight hit the skin, they trigger the release of nitric oxide that has been stored there. This nitric oxide then enters the bloodstream and lowers blood pressure, and it does this independently of any effect on vitamin D (Liu et al., 2014). A large follow-up study of over 340,000 patients confirmed this at population level: more sun exposure was linked to lower blood pressure and lower rates of death from cardiovascular disease (Weller et al., 2020).
Sunlight and cholesterol: a shared pathway
Both vitamin D and cholesterol are made from the same starting molecule in the skin. When sunlight hits the skin, it converts that molecule into the precursor for vitamin D, effectively diverting it away from the cholesterol production pathway. A clinical trial found that 20 minutes of daily sun exposure significantly reduced total cholesterol and LDL in healthy adults (Patwardhan et al., 2017). This is a simple, accessible mechanism that may help support healthier cholesterol levels, particularly for women whose levels are rising in response to hormonal change.
The body clock: the overlooked pillar of heart health
The cardiovascular system runs on a 24-hour cycle. Blood pressure, heart rate, how easily blood clots, and levels of inflammation all follow a biological rhythm governed by the body's internal clock. When that rhythm is disrupted, whether through shift work, irregular sleep, or exposure to bright light late at night, cardiovascular risk rises consistently.
A 2025 Scientific Statement from the American Heart Association concluded that disruption of the body's circadian rhythms, from both behavioural and environmental sources, is an independent and under-recognised risk factor for heart disease (Knutson et al., 2025). This is particularly relevant during perimenopause, when night sweats and insomnia are common, and disrupted sleep is itself a cardiovascular stressor.
Practical tips for keeping your body clock in good shape
• Get outside in natural light within an hour of waking, ideally most mornings, to anchor your internal clock for the day
• Keep your sleep and wake times as consistent as possible, even at weekends; research suggests this regularity may matter more for cardiovascular health than total hours of sleep
• Reduce exposure to bright artificial light in the evening, especially from screens; blue-spectrum light suppresses melatonin and disrupts the metabolic cycles the heart depends on
• Try to eat meals at consistent times, and where possible, earlier in the day; time-restricted eating aligned with daylight hours has shown benefits for blood pressure and inflammatory markers
PUTTING IT TOGETHER
Morning sunlight anchors the body clock, triggers nitric oxide release from the skin, supports vitamin D production, and may help keep cholesterol in check via a shared biological pathway. For perimenopausal women, whose sleep is often disrupted and whose heart health risk profile is actively shifting, getting outside in the morning is genuinely low-cost, high-value preventive medicine.
Frequently asked questions -
-
Yes. Several large, long-running studies including the SWAN study and the Pittsburgh Healthy Women Study confirm that LDL and total cholesterol commonly rise during perimenopause as oestrogen levels fall. Some researchers consider a rising LDL to be one of the earliest consistent biological signs of the menopause transition. This doesn't mean it should be ignored, but it does mean it should be considered in the context of hormonal change, not just diet and lifestyle.
-
High LDL cholesterol may be a significant risk factor, but it's certainly not the only cause - there is a lot more nuance to this discussion. Research shows that heart disease in women also involves damage to the inner lining of blood vessels, wear to the protective glycocalyx coating, body-wide inflammation, and the loss of oestrogen's protective effects during menopause. Women's cardiovascular risk profile is genuinely different from men's, and a cholesterol test captures only part of that picture.
-
Endothelial dysfunction is when the inner lining of the blood vessels loses its ability to produce enough nitric oxide, making them more prone to inflammation, plaque build-up, and reduced blood flow. It's an early and potentially reversible stage of heart disease, and it's directly affected by the decline in oestrogen during perimenopause.
-
Yes. Research shows that UVA light from sunlight triggers the release of nitric oxide stored in the skin, which enters the bloodstream and lowers blood pressure by relaxing blood vessels. This happens independently of any effect on vitamin D levels, and also supports the health of the vessel lining. BUT - DON’T GET BURNED - Check your skin type with the QIMR Berghofer Skin Risk App.
-
The most commonly reported side effect is muscle pain, weakness, or cramping, which may be linked to the reduction in CoQ10 (a natural substance the body needs for energy production inside cells). Other side effects include a modest increase in the risk of type 2 diabetes and, in emerging research, potential effects on eye pressure. Women in perimenopause may have particular reasons to be aware of the CoQ10 connection, given the additional energy demands that hormonal transition places on the body.
-
Several have solid clinical backing: hibiscus tea for lowering blood pressure, bergamot extract for improving the full cholesterol picture (particularly useful in perimenopausal lipid changes), red yeast rice as a natural cholesterol-lowering agent, soluble fibre from oats and legumes, nitrate-rich vegetables like beetroot, and regular aerobic exercise for blood vessel health.
-
The cardiovascular system follows a 24-hour biological rhythm: blood pressure, heart rate, inflammation, and clotting tendency all shift throughout the day. Chronic disruption of this rhythm through irregular sleep, shift work, or night-time light exposure is consistently linked to higher cardiovascular risk. During perimenopause, when sleep is often disrupted by night sweats, keeping a regular daily rhythm becomes an especially important and practical way to protect heart health.
-
The glycocalyx is a very thin, sugar-based protective coating on the inner surface of blood vessels. It acts as a barrier between LDL cholesterol and the vessel wall, helps control blood flow, and prevents inappropriate clotting and inflammation. When it's damaged, by high blood sugar, inflammation, or high blood fats, the process of plaque formation accelerates.
-
Anderson, J. W., et al. (2000). Cholesterol-lowering effects of psyllium intake. The American Journal of Clinical Nutrition, 71(2), 472-479.
Casula, M., et al. (2017). Statin use and risk of new-onset diabetes. Nutrition, Metabolism & Cardiovascular Diseases, 27(5), 396-406.
Ference, B. A., et al. (2017). Low-density lipoproteins cause atherosclerotic cardiovascular disease. European Heart Journal, 38(32), 2459-2472.
Gimbrone, M. A., Jr., & Garcia-Cardena, G. (2016). Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circulation Research, 118(4), 620-636.
Grimes, D. S., et al. (1996). Sunlight, cholesterol and coronary heart disease. QJM, 89(8), 579-589.
Hirose, A., et al. (2011). Effects of the transition from premenopause to postmenopause on lipids and lipoproteins: Quantification and related parameters. Korean Circulation Journal, 41(2), 82-88. https://pmc.ncbi.nlm.nih.gov/articles/PMC3056255/
Kapil, V., et al. (2015). Dietary nitrate provides sustained blood pressure lowering. Hypertension, 65(2), 320-327.
Kelters, I. R., et al. (2025). Circadian rhythms in cardiovascular disease. European Heart Journal, 46(36), 3532-3548. https://doi.org/10.1093/eurheartj/ehaf367
Khatun, K., et al. (2007). Oyster mushroom reduces blood glucose and cholesterol. Clinical and Experimental Pharmacology and Physiology, 34(7), 1-6.
Khoury, E., Brisson, D., Roy, N., Tremblay, G., & Gaudet, D. (2021). Identifying markers of cardiovascular event-free survival in familial hypercholesterolemia. Journal of Clinical Medicine, 10(1), Article 64. https://doi.org/10.3390/jcm10010064
Knutson, K. L., et al. (2025). Role of circadian health in cardiometabolic health. Circulation, 152, e408-e419. https://doi.org/10.1161/CIR.0000000000001305
Kovacic, S., Habicht, S. D., & Eckert, G. P. (2025). Effects of coenzyme Q10 supplementation on myopathy in statin-treated patients: A systematic review and meta-analysis. Journal of Nutritional Science, 14, Article e72. https://doi.org/10.1017/jns.2025.10043
Libby, P. (2002). Inflammation in atherosclerosis. Nature, 420(6917), 868-874.
Libby, P. (2021a). The changing landscape of atherosclerosis. Nature, 592(7855), 524-533. https://doi.org/10.1038/s41586-021-03392-8
Libby, P. (2021b). Inflammation in atherosclerosis: No longer a theory. Clinical Chemistry, 67(1), 131-142. https://doi.org/10.1093/clinchem/hvaa275
Liu, D., et al. (2014). UVA irradiation of human skin vasodilates arterial vasculature. Journal of Investigative Dermatology, 134(7), 1839-1846.
Lu, Z., et al. (2008). Effect of red yeast rice on coronary events. The American Journal of Cardiology, 101(12), 1689-1693.
Manzoni, M., & Rollini, M. (2002). Biosynthesis of statins by filamentous fungi. Applied Microbiology and Biotechnology, 58(5), 555-564.
Matthews, K. A., et al. (2001). Change in cardiovascular risk factors during the perimenopause and postmenopause and carotid artery atherosclerosis in healthy women. Stroke, 32(5), 1104-1111. https://doi.org/10.1161/01.STR.32.5.1104
Matthews, K. A., et al. (2017). Lipid changes around the final menstrual period predict carotid subclinical disease in postmenopausal women. Menopause, 24(3), 277-284. https://pmc.ncbi.nlm.nih.gov/articles/PMC5183479/
McKay, D. L., et al. (2010). Hibiscus sabdariffa L. tea lowers blood pressure. The Journal of Nutrition, 140(2), 298-303.
Mollace, V., et al. (2011). Hypolipemic and hypoglycaemic activity of bergamot polyphenols. Fitoterapia, 82(3), 309-316.
Mundal, L., Sarancic, M., Ose, L., Iversen, P. O., Borgan, J.-K., Veierod, M. B., Leren, T. P., & Retterstol, K. (2014). Mortality among patients with familial hypercholesterolemia: A registry-based study in Norway, 1992-2010. Journal of the American Heart Association, 3(6), Article e001236. https://doi.org/10.1161/JAHA.114.001236
Mundal, L., Igland, J., Ose, L., Holven, K. B., Veierod, M. B., Leren, T. P., & Retterstol, K. (2017). Cardiovascular disease mortality in patients with genetically verified familial hypercholesterolemia in Norway during 1992-2013. European Journal of Preventive Cardiology, 24(2), 137-144. https://doi.org/10.1177/2047487316676135
Pan, S. Y., et al. (2025). Association between statin use and glaucoma risk. Investigative Ophthalmology & Visual Science, 66(15), 7. https://doi.org/10.1167/iovs.66.15.7
Patwardhan, V. G., et al. (2017). Sunlight exposure versus vitamin D supplementation on lipid profile. Indian Journal of Endocrinology and Metabolism, 21(4), 586-590.
Ridker, P. M., Everett, B. M., Thuren, T., MacFadyen, J. G., Chang, W. H., Ballantyne, C., Fonseca, F., Nicolau, J., Koenig, W., Anker, S. D., Kastelein, J. J. P., Cornel, J. H., Pais, P., Pella, D., Genest, J., Cifkova, R., Lorenzatti, A., Forster, T., Kobalava, Z., ... Glynn, R. J. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease. New England Journal of Medicine, 377(12), 1119-1131. https://doi.org/10.1056/NEJMoa1707914
Ross, R. (1999). Atherosclerosis: An inflammatory disease. New England Journal of Medicine, 340(2), 115-126. https://doi.org/10.1056/NEJM199901143400207
Weller, R. B., et al. (2020). Does incident solar ultraviolet radiation lower blood pressure? Journal of the American Heart Association, 9(5), e013837.
Wildman, R. P., et al. (2004). Lipid changes during the menopause transition in relation to age and weight. American Journal of Epidemiology, 169(11), 1352-1361. https://pmc.ncbi.nlm.nih.gov/articles/PMC2727246/
Yilmaz, O., et al. (2019). The role of endothelial glycocalyx in health and disease. Nature Reviews Nephrology, 15(7), 449-467.
Glossary of key terms
The following terms appear throughout this article. Where they are important to keep, plain-English explanations are provided here for reference.
Apolipoprotein B (ApoB)
A protein that carries LDL cholesterol through the bloodstream. Some researchers consider it a more accurate marker of cardiovascular risk than LDL alone.
Atherosclerosis
The gradual build-up of plaques (made of fat, cholesterol, and other substances) inside artery walls, which can narrow or harden arteries over time.
Circadian rhythm
The body's internal 24-hour clock, which regulates sleep, hormones, metabolism, and many other biological processes, including cardiovascular function.
CoQ10 (Coenzyme Q10)
A natural substance produced by the body that plays a vital role in energy production inside cells. Statin medications reduce the body's CoQ10 levels as a side effect.
Endothelium
The very thin layer of cells lining the inside of blood vessels. A healthy endothelium produces nitric oxide and plays a key role in keeping vessels flexible and free of inflammation.
Endothelial dysfunction
When the endothelium loses its ability to function properly, particularly its ability to produce adequate nitric oxide. Considered an early, potentially reversible stage in the development of heart disease.
FSH (Follicle-Stimulating Hormone)
A hormone produced by the brain that stimulates the ovaries. FSH levels rise as ovarian function declines during perimenopause and are one of the earliest measurable signs of the transition.
Glycocalyx
An ultra-thin, sugar-based protective coating on the surface of endothelial cells. It acts as a barrier between LDL and the vessel wall, and is vulnerable to damage from high blood sugar, inflammation, and high blood fats.
HDL cholesterol
Often called 'good' cholesterol. HDL carries cholesterol away from the arteries and back to the liver. Higher levels are generally associated with lower cardiovascular risk.
HMG-CoA reductase
The key enzyme in the liver's cholesterol-making process. Statins and some natural compounds (including red yeast rice and bergamot) work by blocking this enzyme.
LDL cholesterol
Often called 'bad' cholesterol. LDL carries cholesterol through the bloodstream to cells, but when levels are high and the vessel wall is vulnerable, it can accumulate and contribute to plaque formation.
Macrophage
A type of immune cell that plays a central role in inflammation. In the artery wall, macrophages engulf oxidised LDL and can become 'foam cells', a key component of arterial plaques.
Mendelian randomisation
A research method that uses naturally occurring genetic variations as a way of testing cause and effect. Used in cholesterol research to establish whether high LDL actually causes heart disease (not just correlates with it).
Mevalonate pathway
The biological pathway the liver uses to produce cholesterol. Statins block a key step in this pathway; CoQ10 is also made via the same route, which is why statins can reduce CoQ10 levels as a side effect.
Nitric oxide (NO)
A gas produced naturally by the endothelium. It relaxes and widens blood vessels, reduces inflammation, and prevents inappropriate clotting. Production falls with age, hormonal decline, and poor lifestyle factors.
Oxidative stress
An imbalance between harmful molecules (free radicals) and the body's ability to neutralise them. Oxidative stress damages cells and tissues, including the endothelium and LDL cholesterol, contributing to plaque formation.
Perimenopause
The transitional phase before menopause, typically beginning in the mid-40s, during which oestrogen levels fluctuate and begin to decline. It can last several years and is associated with a range of symptoms and metabolic changes.
Pleiotropic effects
Secondary benefits of a drug that go beyond its primary intended action. Statins, for example, have pleiotropic effects including anti-inflammatory and plaque-stabilising properties, over and above their cholesterol-lowering action.
Triglycerides
A type of fat found in the blood. Levels often rise during perimenopause and with high-sugar diets, and elevated triglycerides are an independent risk factor for cardiovascular disease.
UVA
A type of ultraviolet radiation from sunlight that penetrates the skin and triggers the release of stored nitric oxide, independently of vitamin D production.